| << Various and Sundry | Use Ctrl + or – to enlarge or reduce text size. |
The following is from the book The Search for Bridey Murphy. [1] What was a footnote in the original I’ve inserted in the body of the text.
Now how did that amazing machine work?From a reprint of a New York Times article I had learned that a New York doctor had conceived the idea of an equalizing pressure chamber which enables the patient to stop breathing!
...
... Understand that it is not like an iron lung. The chest doesn’t budge; the lungs make no movement; breathing actually stops. The chamber is designed so that an equal pressure is maintained on both sides of the chest, and also on the upper and lower surfaces of the diaphragm. Then, by manipulating the pressures within both the body and head compartments of the chamber, oxygen is brought into the lungs and carbon dioxide eliminated. The volume within the lungs is kept constant, but the density changes. All this without taking a single breath!
Footnote: The doctor who originated this therapy is quoted as saying, “The effect of cessation on the central nervous system is of considerable interest. The impulse for movement in the voluntary muscles in the extremities is strikingly diminished. The patient may lie in the chamber for hours without moving his hands or changing his position. The desire to smoke disappears when voluntary respiration stops, even in patients who have been accustomed to smoke two packages of cigarettes daily. In many instances the relaxation is of such a nature that the patient does not require amusement. ...”When company business next sent me to New York, I took advantage of my first free hour to rush to the office of the doctor who had created the pressure chamber. ...
Within a few days ... my wife and I were standing before a casket-like affair at a hospital in New York City. ... With us were two doctors, researchers at the Columbia University division of the hospital and old hands with the pressure device. “Are you sure you want to enter the chamber?” one of the doctors asked. ...
“Why do you ask?” was my question. ... “Will this machine give me a rough time?”
“No, not at all,” he replied. “But some people have claustrophobia to varying degrees, and so they are terrified at the prospect of being closed up in narrow compartments.”
I wondered whether I had claustrophobia, decided I didn’t, and crawled into the chamber. It is a sort of horizontal cylindrical structure with a dome which slides forward like that over the cockpit of a jet plane. But in this cockpit you stretch out flat on a surface made comfortable by a mattress. Then a partition, like a collar, slides down around the neck, separating the head and the body into two compartments. The dome is pulled back, closing the chamber, and the air compressor is switched on.
At the start I had been told to inhale each time the doctor — I could see him easily through the Plexiglas dome — raised his hand and to exhale as he lowered it. As his hand movements shortened, my respiration was to become shallower until he finally made a crosswise motion with his hands, like an umpire gesturing “safe.” At this point I was to stop breathing entirely.
I did. It was a pleasant, soothing sensation; I didn’t breathe for more than five minutes. It was probably the only five minutes during my entire lifetime when I made no movement whatsoever.
The book I just quoted from does not tell who the doctor was that the New York Times had interviewed, or the date. I located the article, and it was Dr. Alvin L. Barach of the College of Physicians and Surgeons in New York, in Chicago on Jan. 31, 1947. [2]
The machine was actually built by John Emerson (“Jack”), in Cambridge, Massachusetts, and the basic idea behind it was due to Torsten Thunberg in Sweden. However Thunberg’s machine did not stop muscular breathing completely. Barach saw how this flaw might be corrected and Emerson got Barach’s refinement to work.
The following is from the transcription of a talk Emerson gave at Massachusetts General Hospital in 1985, reminiscing about his career inventing and manufacturing respirators: “Some Reflections on Iron Lungs and Other Inventions.” [3] My bracketed comments clarify the text.
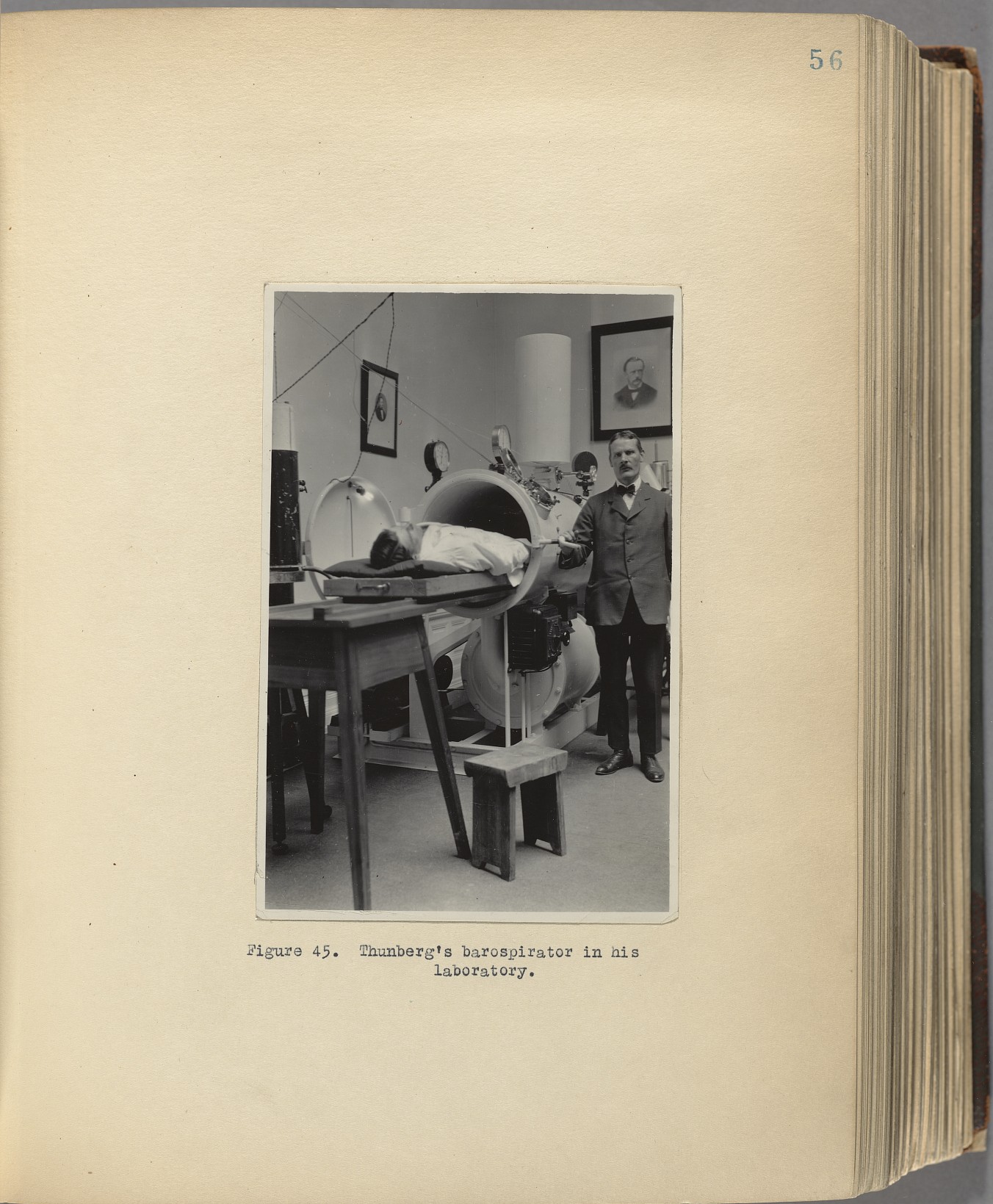
[Referring to a photo:] This machine, you’d think maybe was an iron lung, but this is for Al Barach. This is one of the most sophisticated things we ever made. That was for treating tuberculosis [to give the lungs a rest so they could have a chance to heal], and the patient was completely enclosed.
The Swedes developed this, a fellow named Thunberg, [4] ... he just put the patients completely in the tank and changed pressures up and down quite rapidly and got ventilation by compression and rarefaction. If you press here [making a gesture] on your chest, and bring equal pressure inside, the lungs won’t move. But you can ventilate [that is, move enough air inside and back outside the lungs to sustain life] if you get enough difference in pressure. [That is, oscillation of both pressures simultaneously, the pressures always being the same inside and outside the lung.]
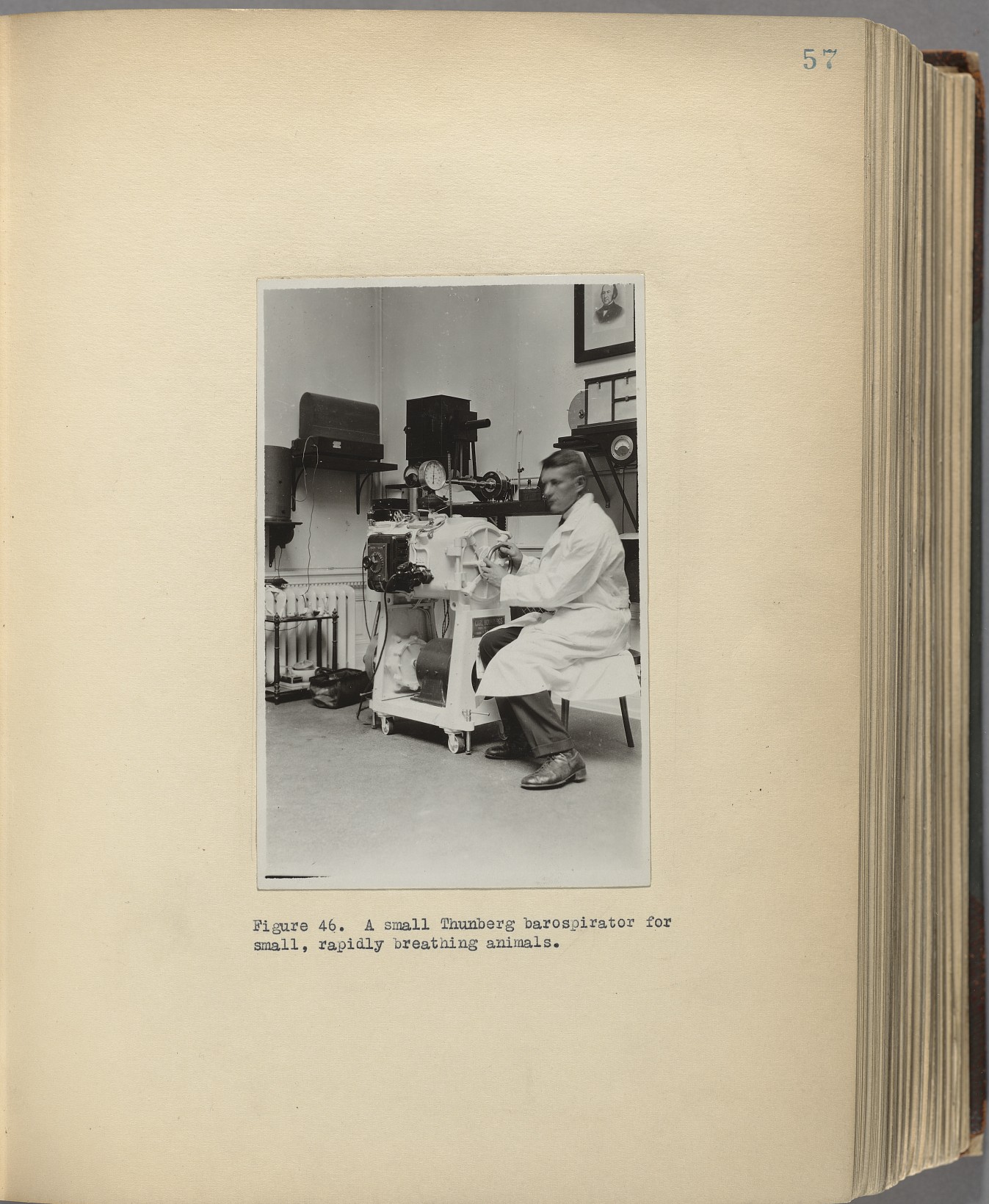
This thing worked, ... for closing — what do you call them — the holes in the lungs [that is, it helped heal tubercular abscesses in the lungs], ... we must have made 60 of those, and just at that time the sulfa drugs were coming, so that [machine] was out the window.
The machine gives air to both the inside and outside at the same time, then takes air from both the inside and outside at the same time. The slight blowing and sucking alternate rapidly; air moves in at high pressure, out at low. Since the pressure remains the same inside and out — though both vary — the chest and lungs never move. You don’t breath (mechanically), yet you breath (respire).
It’s not clear from this description how the two separate compartments, one for the head and one for the body as described in The Search for Bridey Murphy, work into this. A better description is given in the whimsically titled article “Man-Cans” by Julius Comroe in the American Review of Respiratory Disease, 1977; 116:945. We quote:
The Barospirator
In 1926, Thunberg, professor of physiology at the University of Lund, created a device that could arterialize a man’s mixed venous blood without motion of the man’s thorax and lungs. Thunberg called it the barospirator because it worked by producing cyclic pressure changes, not just in the trachea and airways, but around the entire man – both his outside and insides. [a] To accomplish this, the whole man, including head and neck, had to be enclosed in an airtight metal chamber. Then the pressure was cycled from 1 atmosphere to 11 / 6 atmospheres and back to 1 atmosphere, over and over again at the normal rate of the subject’s respiration. If the volume of alveolar gas in the lungs at 1 atmosphere was 3000 ml, the volume stayed at 3000 ml when the pressure in the chamber rose to 11 / 6 atmospheres (because the pressure was now 11 / 6 atmospheres both on the outside of the thorax and in the alveolar spaces) but the number of molecules of O2 and N2 in the alveoli was increased by 1 / 6. In short, the 3000 ml of alveolar gas now contained the equivalent of 3500 ml of air, of which 500 ml was fresh air.Thunberg proposed the alternating pressure sarcophagus as a means of providing an apneic patient with artificial ventilation, and in 1930, Wachenfeldt used a scaled-down Thunberg barospirator to keep alive newborn babies who had no or inadequate ventilation. [b] But the barospirator had a short life because the famous Drinker (or Drinker-Shaw, or Drinker-Murphy) respirator, or “iron lung,” came along three years later and its construction and operation posed fewer mechanical and clinical problems. [c] ...
The Equalizing, Alternating Pressure Chamber
... Barach got his idea of immobilizing lungs from Thunberg and gives him full credit for it. Barach, a clinician and physiologist with a lifetime interest in the diagnosis and treatment of pulmonary disease, had an idea for improving the treatment of pulmonary tuberculosis in the early 1940s, when specific chemotherapy was still 5 or 6 years ahead. Physicians then treated the tuberculous patient with rest. It was a reasonable idea. Skin and muscle wounds healed faster if not subjected to frequent yanking and pulling; why shouldn’t the lesions of pulmonary tuberculosis behave similarly? Some tuberculosis physicians carried the idea to the point of collapsing the lung by pneumothorax or, if adhesions prevented collapse, by collapsing the rib cage surgically (thoracoplasty). Most patients, however, were treated conservatively, with rest. Rest was better than exercise, and enforced strict bed rest was better than a little rest – on the theory that the lower the requirements of the body for ventilation, the less frequent and less extensive would be motion of the lungs and the better the chance for healing.Barach went bed rest one better. He asked: Why not stop the patient’s breathing altogether? Thunberg’s apparatus almost did the trick – by simultaneously compressing the outside and inside of the lungs. Barach tried the Thunberg chamber, but soon noted that thoracic movements didn’t stop completely. Barach then did some animal experiments that showed him why. When the head and body were enclosed in a single airtight chamber and the pressure raised from 1 atmosphere (sea level) to 11 / 6 atmospheres, the increased pressure hit the outside of the thorax with no delay or attenuation, but the same wave going to the alveoli over the nose-mouth-pharynx-larynx-trachea-bronchi-bronchiole route was delayed and diminished by resistance to airflow through the upper and lower airways. If airway resistance was abnormally high, the asynchrony was even greater. Barach’s experiments also showed him how to equalize the pressures reaching the alveoli by the transthoracic and transairway routes – by subjecting the pressure wave hitting the thorax to a resistance similar to the airway resistance. This meant dividing Thunberg’s chamber into two: a head chamber and a body chamber – separated by a rigid collar around the patient’s neck The collar had some holes drilled through it so that the openings between the head and body chambers could be varied in number and area. Barach then applied the alternating pressure waves to the head chamber and when he properly adjusted the openings to the body chamber, the pressure wave hitting the thorax and abdomen matched that reaching the alveoli moment by moment.
He named his new device the “equalizing alternating pressure chamber” or “lung immobilization chamber.” [d] Patients placed in it had no discernible respiratory movements for as long as three hours. By 1940, he had reported on five patients with advanced tuberculosis whose average residence in a chamber was 12 hours per day for 3 ½ months. The only difficulty was that there was no sure way to equalize the air pressure in the patient’s middle ear when pressure waves hit the external auditory canal and the Eustachian tubes 25 times per minute; some drums took quite a beating. [5]
At just about this time, it was becoming possible to treat pneumococcic pneumonia by a very elaborate and costly program of typing pneumococci and then producing in horses type-specific antipneumococcic serum that could be used to combat pneumonia in man. Just as this expensive program was getting underway, it was made obsolete by the clinical use of sulfapyridine (1938) and of penicillin (1941); an inexpensive pill wiped out a huge program to produce antisera. Barach’s immobilization chamber suffered the same fate. Streptomycin and para-aminosalicyclic acid became available in 1945 - 46 and the need for lung immobilization vanished.
That last is a bit premature. Barach and co-workers continued using the “immobilizing lung chamber” into the early 1950s. [6]
The following excerpt describes in more detail the partition between the head and body compartments of the chamber, from “Use of a modified Thunberg barospirator to determine airway resistance in man” by Jules Schwaber and Jere Mead, Journal of Applied Physiology 1968 25(3): 328-332:
Thunberg demonstrated in 1926 that the lungs can be ventilated without accompanying tissue motion by cyclic changes in gas pressure alone. He called his lung-immobilizing chamber the “barospirator.” It was used by Barach to produce lung “rest” in patients with cavitary pulmonary tuberculosis. With the advent of antimycobacterial chemotherapy, the barospirator became obsolete for therapeutic purposes, but it remains a useful device for physiologic experimentation. ...
...
... During immobilization [of the lungs and chest wall during ventilation] alveolar pressure is equal to the pressure inside the chamber at the surface of the body (vide infra) and the latter can be readily measured during airflow....
METHODS
The apparatus consists of two compartments, a head and body compartment separated by a fine-mesh electroplated nickel screen. (Footnote: Catalogue 125P Perforated Products, Inc., Brookline, Mass. Conical openings, hole diameter .003 inch; plate thickness .002 inch. Open area 14.5% nearest U.S. mesh equiv. 200. R = 1.0 inch. H2O / 62 linear ft / min.) The screen is mounted within a vertically movable Plexiglas frame. The frame has a lower border of urethane foam padding and can be adjusted to form a tight fit around the subject’s neck. The screen has linear resistance characteristics.Room air is cyclically pumped into and out of the barospirator chamber at alternating pressures of ± 80 cm H2O by a Rootes blower pump at an adjustable cycling frequency (12 - 20 cycles / min). All pressures are delivered to and drawn from the head compartment of the chamber. ... The subject lies supine in the chamber and is instructed to breathe synchronously with the machine and at a given signal to relax completely. During relaxation the adjustable sliding Plexiglas shield can be used to set the area of open screen between the two compartments of the chamber so that virtually all breathing movements ... cease. The pressure in the body compartment must, in this circumstance, be very nearly equal to alveolar pressure throughout the cycle, since any differences between these pressures would result in chest-wall movements. Tidal exchange is obtained by alternate compression and decompression of gas within the alveoli and airways.
Here is another account, from “Lung Immobilization Chamber Therapy in Chronic Pulmonary Tuberculosis (With Case Reports)” by William Grosfeld and James C. Nash in Chest 1952; 21(3):296-314:
The patient lies in an enclosed chamber in which air can be alternately compressed and decompressed at differential pressures of 55 to 60 mms. of mercury and at a rate of 25 to 30 times a minute, resulting in a tidal flow of 300 to 500 ml. of air in and out of the lungs. The body compartment of the chamber is separated from the head end by a movable partition which lowers over the neck to produce differential pressures between 4 and 12 cm. of water in the head compartment. The addition of this pressure to the compression (positive) cycle of air as it enters the head compartment is adequate to overcome the resistance of the tracheobronchial tree, thus allowing equal air pressure to be simultaneously applied to the inner and outer surfaces of the chest wall as well as the upper and lower surfaces of the diaphragm. The immobilizing chamber is air conditioned. The head compartment is equipped with a two-way communication device. A light for reading and a small battery radio may be placed beside the head. By means of a release catch the patient may enter and leave the chamber without help. ... By proper training, most patients learn to immobilize their chest wall and diaphragm in the first week of practice, thereafter the chest is immobilized without conscious or voluntary effort. With an occasional patient claustrophobia is a deterrent to complete immobilization; in others, nervousness and inability to relax prohibit lung immobilization.
As Comroe notes in the quote previous to the above two, Thunberg’s invention (in 1924) actually preceded the invention of what came to be known as the iron lung, which does move the lungs. See “Experiences in the Treatment by the Barospirator” by Paul W. Fritsch, Acta Medica Scandinavica, 1932, vol. 78. This article begins:
Among the numerous methods of artificial respiration from older and more recent times the treatment by the barospirator occupies a place by itself. All other methods try to imitate the natural respiration by either rhythmically expanding and compressing the chest or by insufflating it with a quantity of gas necessary for ventilation. ... As late as in 1929 Drinker and McKhann and Wachenfeldt in 1930–31 published descriptions of apparatus in which the patient rests with his head outside, and where the chest movements are brought about by pressure changes in the external air. ...
In principle the above-mentioned methods concur in that they all aim at volumetric changes in the lungs as nearly normal as possible.
Thunberg’s barospirator (1924) works on a different principle. ...
The following is from “The development of apparatus for intermittent negative pressure respiration” (Part 2: 1919-1976) by C. H. M. Woollam in Anaesthesia, 1976, Volume 31, pages 666:
Scandinavia. Thunberg’s Barospirator tank (1920)One type of tank respirator, introduced in Scandinavia, worked on different principles from the rest. Dr. T. Thunberg had been developing his ‘Barospirator’ for 20 years when the final design was produced in the 1920’s ... . The whole patient was placed in the tank (later versions were room sized to take medical staff as well).
The air pressure in the tank was raised and lowered rhythmically by the attached cylinder. The changing air pressure caused a pressure difference from outside the patient to the lungs; the pressure change altered the volume [rather mass, or density] of air, which then flowed in and out of the lungs without moving the chest wall.
Thunberg and his colleagues published many articles on the use of the ‘Barospirator’ in poliomyelitis, drug overdose and various respiratory diseases. The results of treatment by the ‘Barospirator’ were poor and it never became popular outside Scandinavia.
See also “Treatment of Respiratory Failure in Acute Epidemic Poliomyelitis” by M. Bernard Brahdy and M. Lenarsky, American Journal of Diseases of Children, 1933, vol. 46, no. 4, p. 705-729. This article begins somewhat inaccurately because, as noted in the quote above, the physics of the Thunberg respirator is quite different from that of the later iron lung (what they have in common is the use of a body enclosure, full in the case of Thunberg’s machine, excluding the head in the case of the iron lung). Also, it claims that the Drinker respirator was based on Thunberg’s. I haven’t looked into this detail but I think the Drinker respirator was developed without knowledge of Thunberg’s.
Respiratory failure occurs in poliomyelitis when the disease damages the motor nerves controlling the muscles involved in breathing. Neither these muscles nor the lungs want rest, indeed their movement should be encouraged. Thus in the case of poliomyelitis the iron lung would be superior to the barospirator. But in cases where the lungs need rest the barospirator comes into its own.The barospirator for artificial respiration designed by Thunberg [e] served as a basis for the construction of the respirators now used in many hospitals for the treatment of respiratory failure ... . In the Thunberg barospirator the patient was entirely enclosed in an air-tight cylinder. The air pressure within this cylinder was alternately raised and lowered, resulting in an intrapulmonary exchange of air sufficient to maintain life for long periods. Thunberg aptly described the effect of the barospirator on the patient as resulting in respiration without respiratory movement.
It soon became evident that this ingenious apparatus was not satisfactory for cases of prolonged respiratory failure. Drinker and Shaw [f] modified the barospirator so that the patient’s head would be outside the air-tight cylinder. This is the apparatus most frequently used for respiratory failure in poliomyelitis.
I wouldn’t mind trying one of the later Thunberg-Barach-Emerson machines. In the meantime I’ll just have to hold my breath.
Postscript: A word about dead space. “Dead space” is the technical term for the interior volume of the conducting airways of the lung. Air that remains in the dead space does not reach the alveoli and hence does not take part in gas exchange. (For a good idea of what dead space means consider a snorkel tube, which increases the dead space artificially. Now imagine it becoming longer, increasing the dead space. At some point it would be so long that no fresh air at all reaches the business part of the lung.) Now in a barospirator, though the frequency of the pressure change is high its amplitude is low, but apparently high enough that it refreshes more than dead space air. One reference (see above) says the barospirator provides a tidal flow of 300 to 500 ml of fresh air into and out of the lungs. Another way fresh air could get to the alveoli is by diffusion and turbulence but none of the above referenced articles mention it.
{kind=link}
{kind=link}